Buvidal vs Methadone: Which is the Better Opioid Treatment?
April 30, 2024
3:42 pm

Table of contents
- What Buvidal Does when considering Buvidal: alternative to Methadone?
- Buvidal: alternative to Methadone? Considerations
- Managing Expectations with Buvidal: alternative to Methadone?
- Potential Pitfalls
- Buvidal: alternative to Methadone? Conclusion
- Get Free Advice From an Experienced Addictions Clinician on Buvidal: alternative to Methadone?
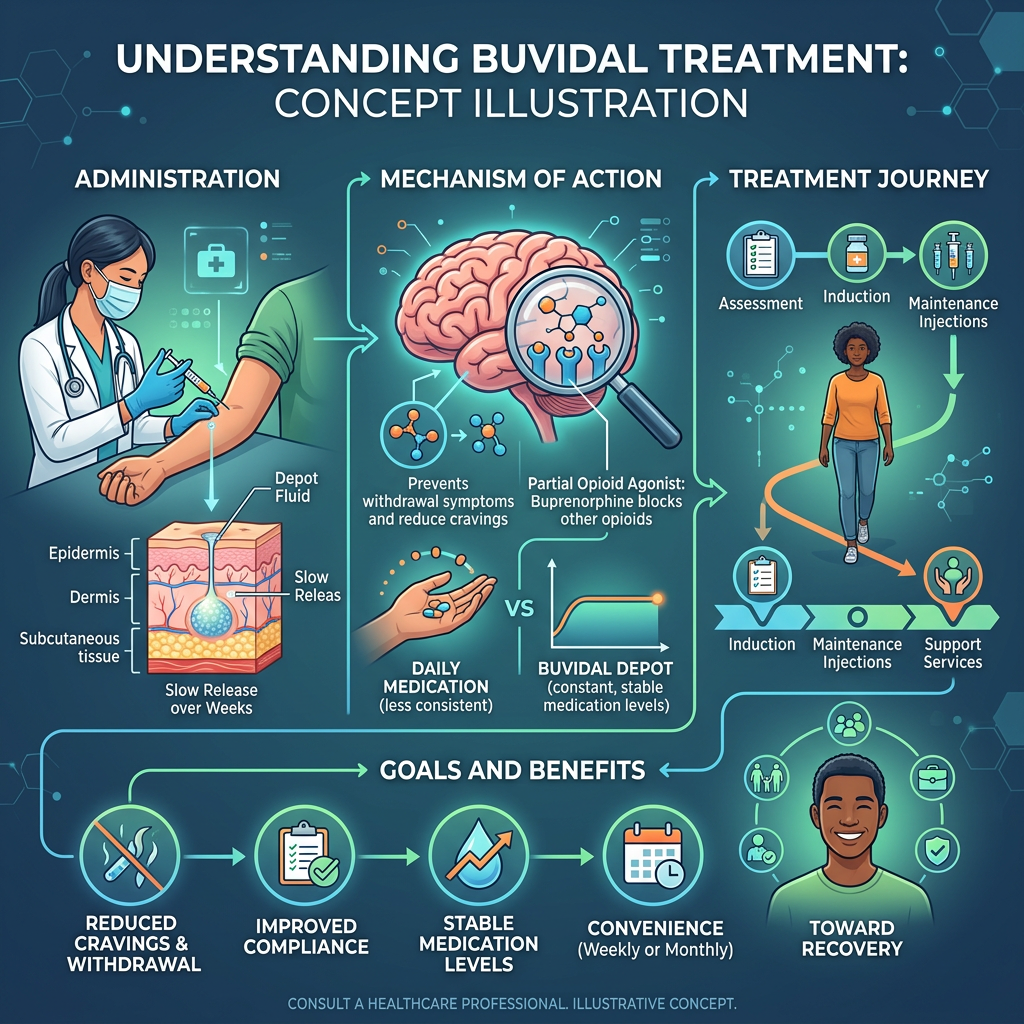
Buvidal: alternative to Methadone? It certainly can be.
Buvidal is, quite simply, injectable Buprenorphine.
In fact, for many seeking Buvidal as an alternative to Methadone, the appeal lies in receiving an intramuscular injection, usually in the upper arm, which replaces the need to attend a chemist on a daily/weekly/ fortnightly basis.
Different services use different protocols for prescribing it. Typically, they administer a 16mg injection in week one, repeat it for four weeks, and then continue with a monthly injection. But is Buvidal truly an alternative to Methadone?
What Buvidal Does when considering Buvidal: alternative to Methadone?
As Buvidal is Buprenorphine, a patient needs to be in withdrawal before commencing treatment.
While it is not dangerous to give it if someone is not, it will cause withdrawal as it will force opioids from the receptors in the brain.
When people ask about Buvidal: alternative to Methadone, these distinctions matter.
People know this as precipitated withdrawal.
For those who have never used buprenorphine before, it is good practice to give the patient a small dose of oral buprenorphine first, especially for anyone weighing Buvidal against Methadone as an alternative, to ensure there are no issues.
Application
Healthcare providers administer a 4mg sublingual tablet or oral dispersible tablet.
They then ask the patient to remain in the waiting room for one hour to measure and observe any side effects.
These steps are important when considering Buvidal as an alternative to Methadone
The usual practice is for clients to use oral buprenorphine (Subutex/Espranor) for two weeks, 1st, before moving to Espranor.
Those comparing Buvidal against Methadone should note these preliminary steps as part of the alternative pathway.
This is to build on a therapeutic relationship and observe for adherence to treatment (urine drug screening).
Buvidal is relatively expensive, with a single injection costing several hundred pounds.
This cost raises questions for patients considering Buvidal as an alternative to methadone.
Oral Buprenorphine is, relatively, inexpensive compared to Buvidal as an alternative to Methadone for patients seeking cost-effective options.
Buvidal: alternative to Methadone? Considerations
While there are some obvious advantages to Buvidal such as no risk of diversion and assurance that the patient has had treatment, there are some considerations.
Also, the difference between Buvidal as an alternative to Methadone is clear when assessing the “dampening” effect that Methadone provides.
Dampening is when Methadone (when taken at therapeutic doses) stops someone feeling the effects when taking “on top” opioids (opioids in addition to Methadone). For those considering Buvidal: alternative to Methadone?, this effect is unlikely to be replicated, making it a unique option.
While it is possible to have the injection a day or two either side of the due date, there is the risk that patients will stop engaging because it is an injection and it is “in their system.”
This highlights an important limitation for those considering Buvidal as an alternative to Methadone?
Managing Expectations with Buvidal: alternative to Methadone?
However , from what clinicians have seen when prescribing Buvidal, is that patients are expecting it to do things it simply can not do.
In essence, it is not magic and is merely an injectable form of an existing drug: Buprenorphine.
However, patients can be assertive in their demands to try it, especially when they are already on Methadone. And therein lies the most difficult problem for anyone evaluating Buvidal: alternative to Methadone as a treatment.
Patients can only transfer to Buvidal when they are on 30MG of Methadone, and coming down on Methadone is a marathon: not a sprint.
This slow process is crucial when discussing Buvidal as an alternative to Methadone?
Some clients will become overly focused on Buvidal and attempt to switch more quickly by either stopping their Methadone or reducing very quickly, especially those interested in Buvidal as a possible alternative to Methadone.
Key Takeaways on Buvidal: alternative to Methadone?
- Buvidal is an injectable form of Buprenorphine and may be seen as an alternative to Methadone due to its administration method.
- It is crucial for patients to be in withdrawal before starting treatment to avoid precipitated withdrawal effects.
- While Buvidal eliminates the daily need to visit a pharmacy, it is relatively expensive compared to oral Buprenorphine options.
- Considerations include the dampening effect that Methadone provides, which Buvidal may not replicate.
- Patients should collaborate with clinicians for informed decisions about Buvidal: alternative to Methadone?

Potential Pitfalls
This puts the patient at risk as their tolerance will drop and there is the additional risk of craving: A, potentially, dangerous combination.
Furthermore, for clients who are alcohol dependent and/or using large amounts of gabapentinoids and benzodiazepines, Buvidal is not a realistic option as Naloxone will prove far less effective than it would against Methadone toxicity.
Clearly, treatment plans are made collaboratively between a patient and their clinician.
For those who are not sensitive to Buprenorphine, Buvidal can provide a useful method of delivering Opioid Substitution Treatment (OST), especially for those in rural areas and with complex, poly substance, dependencies.
Both statutory services and fee-paying patients face cost considerations and risk quickly losing their current treatment plans when switching to Buvidal, especially those considering Buvidal as an alternative to Methadone.
Buvidal: alternative to Methadone? Conclusion
Researchers first patented buprenorphine in 1965 and licensed it for use in America starting in 1981.
Today, many people with opioid dependency widely use it. Buvidal is, merely, the same drug in an injectable form.It certainly has its uses, but patients should make informed choices in collaboration with their clinicians and avoid being swayed by others or what they read online.
If you are considering Buvidal: an alternative to Methadone, call and speak to an experienced addictions clinician who has treated many patients with this drug.
Get Free Advice From an Experienced Addictions Clinician on Buvidal: alternative to Methadone?
You can get free advice from an experienced addictions clinician in complete confidence.
We do not charge for treatment referrals.
We only signpost to legally registered centres.
Our service is registered with the Information Commissioners Office.
Need help finding the right rehab for you or a loved one? Get in touch today and take the first step toward recovery.
Speak to usRecent Posts
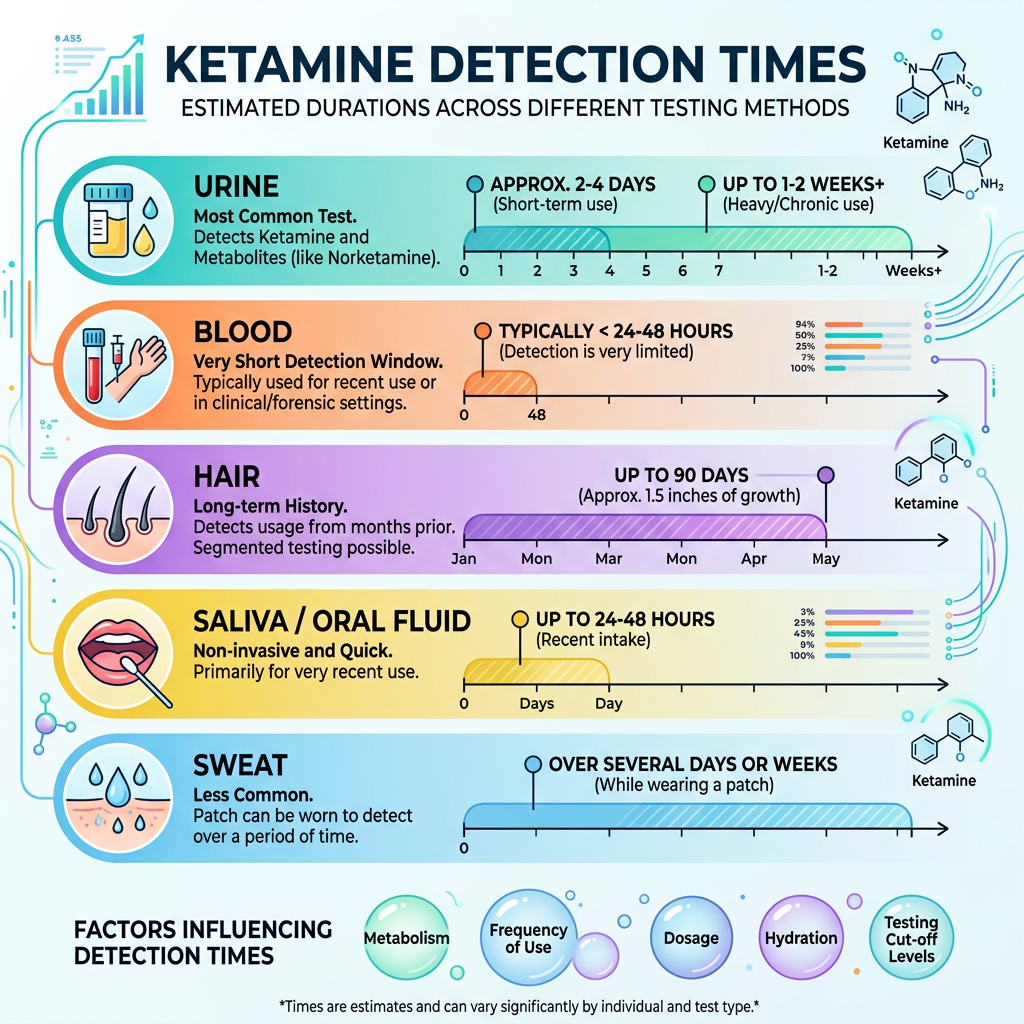
How long does Ketamine stay in your system?
How long does Ketamine stay in your system? As an experienced addictions clinician with over thirty years experience my question to that is: Why do you need to know? Is it because you are worried it will show up in a drug screen at work? Are you worried about being drug tested by the police…
Grace Kennedy
12:23 pm, July 2, 2026
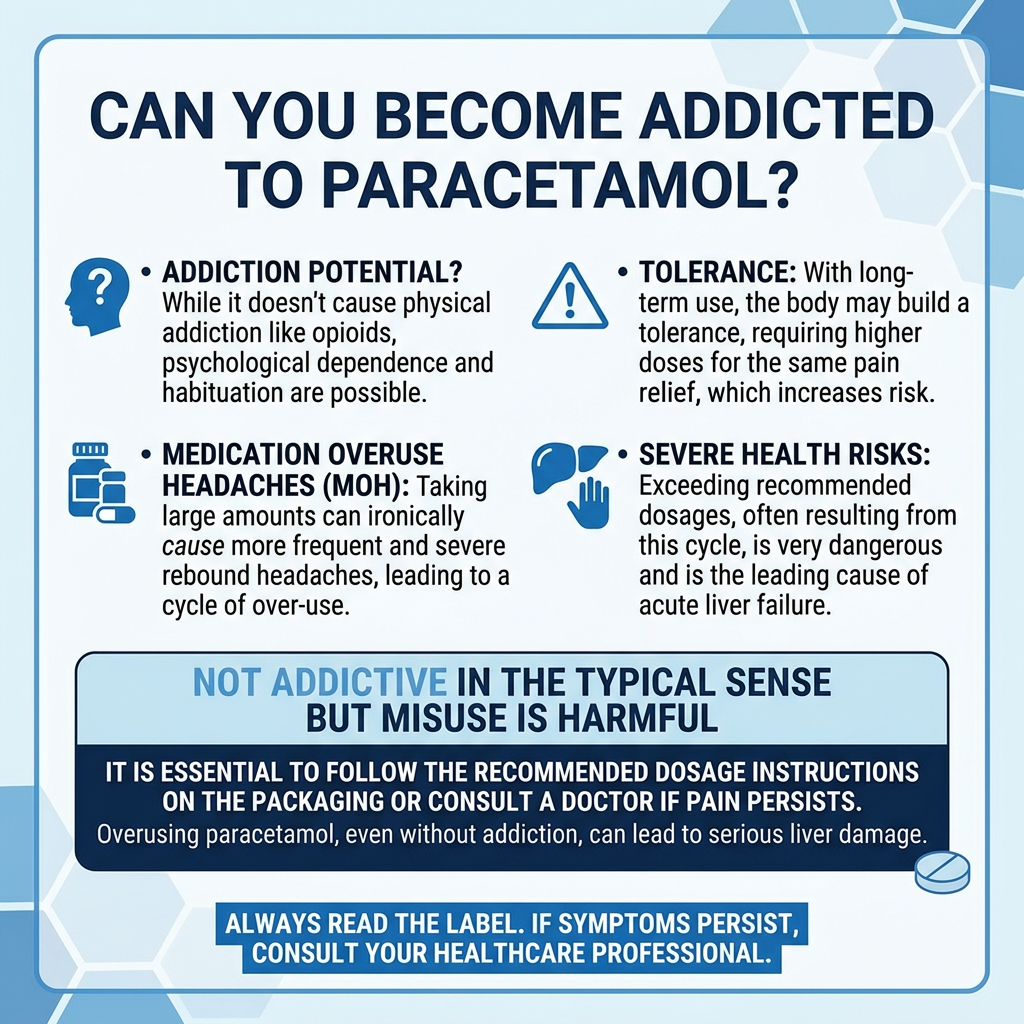
Can you become addicted to Paracetamol?
Can you become addicted to Paracetamol? No. Well not it in the same way you become addicted to heroin or alcohol as the way it affects the brain is different. That doesn't mean that some people are not addicted to taking it in the way that they take it, repeatedly. How does Paracetamol work? The…
Grace Kennedy
6:08 pm, June 26, 2026
Can you do a Methadone detox at home?
Can you do a Methadone detox at home? In theory: Yes. In practice: No. It is a nice idea that you can stay at home, take some methadone and your opioid use disorder is cured. Sadly it just doesn't work like that. In order to understand why this won't work you need to know what…
Grace Kennedy
6:49 pm, June 25, 2026